Electrophysiology surgery (washingtonhra.com)
[Worldtrippers home] [Mountaintop home]
Electrophysiology surgery (washingtonhra.com)
As usual, we’re posting this detailed information for anyone out there who may have a similar condition and wants to know more.
For almost 40 years, Russell has had a heart condition called supraventricular tachycardia or SVT. “Tachycardia” means a rapid rhythm of the heart. “Supraventricular” means that it originates above the ventricle area of the heart.
The heart is composed of four chambers that contract regularly, filling your blood with oxygen and sending it off to the rest of your body. These contractions are caused by two nodes that send electrical impulses, causing your heart to beat regularly.
This graphic shows the four chambers of the heart, as well as the two electrical nodes that make it beat. (drmiri.com)
Here’s an animated graphic! (wikipedia.org)
With SVT, Russell’s heart has an extra electrical circuit. This accessory pathway alters the heart’s normal electrical system. While a normal heart beats 60 times a minute, Russell’s can suddenly and inexplicably start beating at 220. The rapid palpitations make his heart less effective, reducing blood flow and blood pressure. Spells can start at any time and last from a few seconds to several hours.
(One high point – or low point – of Russell’s SVT life was when he had to be airlifted off of Mount Shasta in a medical helicopter a few years ago.)
A normal heartbeat compared to an SVT heartbeat (engr.wisc.edu)
Since adolescence, Russell has controlled – but not eliminated – his SVT with various beta blocker medications. About 15 years ago, a new medical field called cardiac electrophysiology was developed. Russell’s cardiologist told him about a new medical procedure, RF catheter ablation, that could potentially fix his heart.
The surgery had an 85 percent success rate. Russell wondered what happens during the other 15 percent. Afraid of death or a permanent pacemaker, Russell chickened out and declined.
This summer, we watched our son Joss go through his second major surgery in three years. Russell decided he had no excuse for chickening out of his own minor surgery. If Joss could do it, so could his dad! Russell scheduled a catheter ablation for September 7, after the long Labor Day weekend.
The only preparation was fasting the night before the surgery. Russell would go into the hospital first thing in the morning and be home by that evening. The operation itself would take two to four hours, followed by several hours of recovery. Gail would drive him to and from the hospital and stay with him all day.
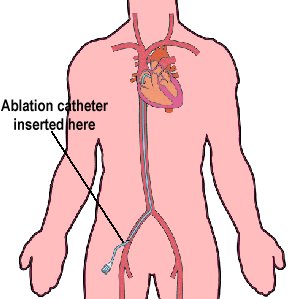
In a catheter ablation, the patient remains conscious, but extremely groggy. A series of catheters, or thin wires, are inserted into a major artery in the groin area and fed all the way up into the heart. They are placed inside the heart at various locations and used to stimulate heart palpitations. A number of monitors try to capture exactly where the palpitations originate from.
An electrophysiology operating room. This photo is from Mount Auburn Hospital, but it is very similar to the setup at Kaiser Santa Clara. The large apparatus is a fluoroscope that captures real-time X-rays. (inventorspot.com)
Depending on where the accessory pathway is, additional catheters may need to be inserted in the leg vein (to reach the other lateral side of the heart) or the neck (to reach the upper half of the heart). Finally, RF (radio frequency) energy is directed to the tip of the appropriate catheter. This disables – or ablates – the problem cells, permanently destroying them.

Catheters are inserted into major blood vessels near the groin, then fed all the way up into the heart. (washingtonhra.com and wolfminimaze.com)
Here’s another animated graphic! (washingtonhra.com)
As we were later told, Russell had a specific form of paroxysmal SVT, a variation of Wolff-Parkinson-White syndrome.
“WPW is a disorder of the heart in which the ventricles of the heart contract prematurely due to an accessory pathway known as the bundle of Kent. This accessory pathway is an abnormal electrical communication from the atria to the ventricles. The incidence of WPW syndrome is between 0.1% and 0.3% of the general population.” (wikipedia.org)
Wolff-White-Parkinson syndrome (wikipedia.org)
Russell’s specific case was a concealed left lateral bypass tract.
“Although AV accessory pathways usually conduct antegradely and retrogradely, some AV bypass tracts are capable of propagating impulses in only one direction. Bypass tracts that conduct only in the retrograde direction occur more frequently with an incidence reported as high as 16 percent. Because they do not pre-excite the ventricles, the surface ECG during sinus rhythm appears normal and therefore these pathways are called ‘concealed’.” (Chinese Medical & Biological Information: cmbi.bjmu.edu.cn)
Various types of accessory pathways (rjmatthewsmd.com)
Russell ended up needing four catheters in his groin (three in the artery and one in the vein) in addition to one catheter in his neck. Fortunately, he has almost no memory of any of this happening because he was so drugged up.
The operation went off with no complications. The hardest part was that Russell had to lie on a gurney for six hours afterwards without moving his head or his right leg. (This was to give his blood vessels time to close up.) He ended up being the last patient in the cardiac recovery ward – they were shutting off the lights when he was finally released at 7:00 pm.
We may not know if Russell has been “cured” for several months. In the meantime, he is not supposed to lift anything heavy for about a week. Fortunately, he has Gail to handle all of the “heavy lifting” – in more ways than one!
There is a four-minute educational video that describes the entire RF catheter ablation procedure here at fletcherallen.org.